

For over a year, Americans have been subjected to dizzying whiplash over the many contradictions of the COVID-19 'pandemic'. There have been dizzying flip-flops on almost everything related to it. Masks or no masks? 3 feet or 6? Therapeutics or vaccines? Asymptomatic spread or not. COVID death or motorcycle accident death? Almost zero attention is given to cost-benefit analysis when making so many impactful decisions. Fifteen days to flatten the curve became draconian lockdowns, causing still untold economic, psychological, and human costs. This was an illness that was handled differently, in nearly every way, by our government, the media, and the medical community, with the possible costs still unknown.
An article written for UncoverDC on April 7, 2020, by Celia Farber was one of the first to examine the use of Polymerase Chain Reaction (PCR) testing as a way to diagnose the absence or presence of the virus. It rightly mentions its inventor, Kary Mullis, and explains his findings. The article states:
“PCR is really a manufacturing technique,” Crowe explained. “You start with one molecule. You start with a small amount of DNA, and on each cycle the amount doubles, which doesn’t sound like that much, but if you, if you double 30 times, you get approximately a billion times more material than you started with.
So as a manufacturing technique, it’s great. [What they do is they attach a fluorescent molecule to the double-stranded DNA as it's being produced.] You shine a light at one wavelength, and you get a response; you get light sent back at a different wavelength. So, they measure the amount of light that comes back, and that’s their surrogate for how much DNA there is. I’m using the word DNA. There’s a step in RT- PCR test, which is where you convert the RNA to DNA. So, the PCR test is actually not using the viral RNA. It’s using DNA, but it’s like the complementary RNA. So logically, it’s the same thing, but it can be confusing. Like why am I suddenly talking about DNA? Basically, there’s a certain number of cycles.”
This is where it gets wild.
“In one paper,” Crowe says, “I found 37 cycles. If you didn’t get enough fluorescence by 37 cycles, you are considered negative. In another paper, the cutoff was 36. Thirty-seven to 40 were considered “indeterminate.” And if you got in that range, then you did more testing. I’ve only seen two papers that described what the limit was. So, it’s quite possible that different hospitals, different States, Canada versus the US, Italy versus France are all using different cutoff sensitivity standards of the Covid test. So, if you cut off at 20, everybody would be negative. If you cut off a 50, you might have everybody positive.”
Prior to February of 2021, the CDC generally recommended the cycle threshold at 40 cycles. An abstract from August of 2020 states that "a positive test result was defined as an exponential fluorescent curve that crossed the threshold within 40 cycles (cycle threshold [Ct] <40)."
The latest covid related flip-flop surfaced in February when the CDC quietly released updated guidance on (PCR) testing that was already seemingly suspect in the first place. The reason for the change? Maybe it was because vaccines were now in play.
Per a February 2021 CDC document, clinical specimens for sequencing collected for vaccinated people with "Covid 19 breakthrough cases"—"should have an RT-PCR Ct value ≤28." The purpose of the guidance was to "investigate SARS-CoV-2 infections among people who received COVID-19 vaccine to identify trends or clustering in demographic, the administered vaccine, or the infecting virus."
With the arrival of the various vaccines, the threshold was dropped significantly. In layman's terms, dropping the threshold of cycles will more than likely result in fewer results showing the presence of the virus.
 ZeroHedge Questions
ZeroHedge Questions
The questions that arise from this sudden change are numerous and, to date, unanswered by those in charge. After having spoken with multiple experts working in the medical field, there are some things that are factually true.
UncoverDC interviewed multiple people—two of whom will be quoted below. Source One worked in labs performing PCR tests for seven years, 2 years as a psych nurse, 1 year in cardiac telemetry, 1 year in managed care, and is now three years into a career in process improvement of clinical review processes—a total of 14 years in the medical field.
Source Two is a nurse who has been in the field since 2013. Sadly, neither is willing to go on the record because of how highly politicized this virus has become—which in itself seems to be very telling. Below are some of the findings and questions that we all should be examining:
- Source Two, the nurse, stated that she was willing to give Fauci and the CDC the benefit of the doubt in the beginning. "Maybe in the beginning, due to the lack of information about the virus, the cycle threshold was understandable." However, she said that by the summer, it should have been obvious that a cycle threshold of 40 was probably too high but then was never adjusted down in the U.S.
- All who were interviewed confirmed Celia Farber's reporting in April that the tests were never designed to diagnose a SARS- CoV-2 infection.
- Plainly stated, it seems that between March and December of 2020, labs in the U.S. were essentially "running as many cycles as necessary to achieve a positive result, despite experts warning that this was pointless (even Fauci himself said anything over 35 cycles is meaningless)"—per recent reporting by ZeroHedge.
- Both experts interviewed told UncoverDC that when one begins to run higher cycle thresholds, the result is often more than likely "noise," leading to false positives. In other words, "when it crosses that threshold, it is pretty much garbage," according to the former lab technician.
The first guidelines for testing were released in January of 2020. The document was relatively unspecific. Cycle thresholds of 35-40 were being used during the period of January through December.
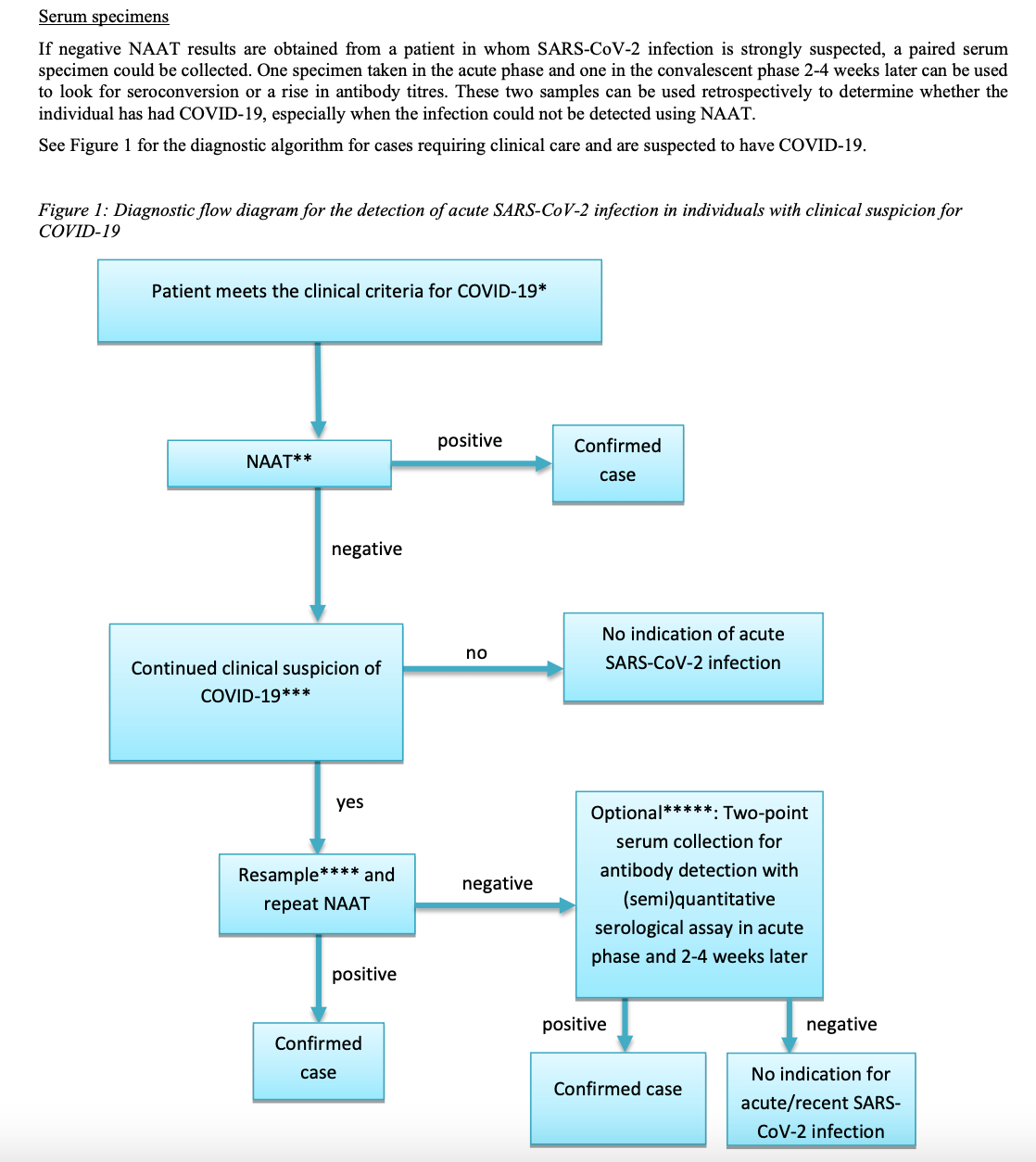
In September, the guidelines seemed to begin to shift in other important areas formerly used in the medical field for such viruses. It seems the World Health Organization (WHO) was recommending a return to the world where other diagnostic criteria could be used to confirm and report a positive COVID-19 result. This "diagnostic flow diagram" appeared in September appeared in their guidance, with very little notice or comment from government officials. Certainly, your average person was unaware of the changes.
 WHO/September
WHO/September
Still, even in the above diagram, at the point where they run a PCR test, they should run another type of test if prior standards and methodologies were to apply. In any other world, according to the former lab technician, "A positive PCR with clinical symptoms of other illness would still be a false COVID positive. And from a diagnostic perspective, you'd rather have a false positive than a false negative. But from the perspective that the data found here would be used to inform the presence of a pandemic, it is misleading.”
On the heels of changes released in December by the CDC, the WHO then released guidelines in early January of 2021 asking labs to use manufacturers' standards for the cycle threshold. Suddenly, in January, the WHO is explicitly asking technicians to follow the Instructions for Use (IFU) provided by the manufacturers of the PCR assays. Prior to December, there was no such language. The cycle thresholds used were not being requested to be provided with the tests used to diagnose for a positive COVID-19 result. Of note, Florida mandated reporting of cycle threshold values in December.
 WHOManufacturers' guidelines
WHOManufacturers' guidelines
The question we may want to ask ourselves here is the following: if you are shifting the cycle thresholds, what are the real-world consequences of the shifts, and what is happening at the same time those cycle thresholds are being shifted?
The timing of the change to Ct value of ≤28 for a vaccinated individual is, at best, suspicious and at worst political. Lowering the threshold means you may not pick it up if you are comparing it to what the CDC has been recommending. More importantly, one would be hard-pressed to find protocols that "used one standard of testing for vaccinated people and another for the rest of us," according to the nurse interviewed.
Even more important is the thought that, if the CDC is recording cases using the data collected between March and December as the standard, but now anything over 28 won't be recorded for the vaccinated, is the CDC and WHO "going to go back and correct the data you collected during that time period? You simply cannot compare that data to the data being collected after February unless you go back and reassess the data and eliminate samples that are above the current cycle thresholds if that data is even available," stated the former lab technician expert who worked in PCR testing for 7 years.
To be clear, at thresholds of 35-40, you are "overcounting people as sick who tested positive for the virus," and that data is being used to dictate everything we do—whether we re-open schools and businesses, whether we see our grandparents, you name it. The effects of "mistakes" or shifting standards like these have untold and devastating real-world consequences.
The experts interviewed agreed that the test alone should never have been used to diagnose or populate the data being used to inform the public of positive cases in the first place. "A test is a piece of information. We treat patients. Doctors need to use their knowledge and their training, and their clinical judgment. Never in the known history of medical care have we approached an illness in this way. Not only is the test NOT meant to diagnose SARS-CoV-2, it was used almost exclusively to push data about positive cases."
For example, for H1N1, "a positive test result for 2009 H1N1 influenza virus using the DIATHERIX H1N1-09 Influenza Virus Test indicates that the patient is infected with the 2009 H1N1 influenza virus. The test does not indicate the stage of the infection. Laboratory test results should always be considered in the context of clinical observations and epidemiological data in making a final diagnosis."
The test should also be compared to an Antigen test. If you have both the RNA and the antigens present, you have two important components; DNA and proteins. PCR positive specimens should then be cultured for the virus regardless of the threshold being used. "That is the gold standard," continued the former lab technician, "The lab culture should be the gold standard to confirm the presence of the virus." The PCR test should be used as a screening tool, not a diagnostic tool. Again, data from the PCR test alone does not a pandemic make.
Notably, one of the experts referred to a study in So. Korea that found, in his words, "anyone who was objectively paying attention knew in May that individuals who had been tested positive for COVID-19 or had symptoms of COVID-19, could not later spread the illness even if a positive covid test popped up weeks later." Simply stated, through its massive surveillance and tracing programs in combination with the May study, South Korea changed its standards for a COVID-19 diagnosis requiring isolation in May of 2020. No symptomatic spread was happening from previously positive patients. The U.S. has yet to issue the same kind of statement.
It is critical to digest what has been recently posted word-for-word on the CDC's website about the recent changes in standards. With regard to vaccine breakthroughs—the "CDC transitioned from monitoring all reported vaccine breakthrough cases to focus on identifying and investigating only hospitalized or fatal cases due to any cause. This shift will help maximize the quality of the data collected on cases of greatest clinical and public health importance."
Unpack that statement. So now, if you are fully vaccinated, and you supposedly have a breakthrough positive result, unless you are in the hospital dying, you will no longer be counted as a COVID-19 case. Now, apply all of the information above to this statement. Never have two standards of testing been applied—one for the vaccinated and another for everyone else.
The following questions come to mind:
Is the CDC going to go back now and correct the data to make it more useful? In other words, according to the former lab technician, "will the CDC go back and remove all tests with cycle thresholds above 28—if that data is even available—so that the data will reflect an apples to apples comparison of data going forward?"
Will this new lower cycle threshold standard suddenly emerge later as the one to apply to everyone?
Our job and our mission at UncoverDC is to publish thought-provoking information that will help readers question and maybe read more. Our job is to research, ask questions, read studies and source documents, ask experts, and then provide enough information for you, the reader, to begin to ask those questions, and then, maybe even ask some more of your own.
The most important takeaways seem to be these:
All of the experts interviewed told UncoverDC that "never in their experience or even in their training" did they witness the strict protocols (like only using a positive PCR test) to conclude and report that an individual was COVID-19 positive. Never before have protocols remained so stubbornly adhered to while blithely ignoring anecdotal field evidence or legitimate studies and data being shared along the way to inform policy decisions that have potentially devastating implications for how we plan to live our lives.
The experts relayed that the stringent directives were oddly top-down and going to doctors, NOT just nurses. The significance of that information is that nurses usually get those protocols but then doctors, whose training and experience afford them the ability to come in behind them and look at ALL the data and then use their clinical judgment to diagnose and report a positive case or diagnose the individual with said disease.
Alarmingly, many doctors, scientists, and nurses in the field have received such top-down, strident orders that they have been afraid to use the methods they have used before the COVID-19 event for fear they will lose their jobs or their licenses. It seems that all methods, clinical judgment, history about what we know about how viruses behave and are transmitted and collected and reported and resolved in the human body have been scattered to the wind. All prior knowledge and good practices be damned.
Prior to COVID-19, these same nurses and lab technicians were free to practice as trained. PCR should be more of a screening tool, not a diagnostic tool. Prior to COVID-19, they were free to use the PCR as the test for that which it was designed to investigate. Per Kary Mullis—the scientist credited with the invention of PCR—the PCR test is used to "make a whole lotta somethin' out of somethin'. He also said, "The PCR test, if you do it well, you can find almost anything."
Before COVID-19, those in the medical field were free to practice medicine or science in the way that their years of experience informed their practices, diagnoses, and treatments.
As the lab technician explained, "Science is strengthened through scrutiny." In the case of COVID-19, the ability to scrutinize has been all but obliterated. No scrutiny on data. No scrutiny on cycle thresholds. No scrutiny on whether the PCR test should be used at all to diagnose and report. No scrutiny on masks. No scrutiny on distancing. No scrutiny on almost anything, and if scrutiny was applied, a crushing hammer has been soundly applied.
Prior to COVID-19, the therapeutics that were previously available and deemed safe were shuffled away like fugitives in the night and prohibited from use, even though many brave clinicians in the field were prescribing them early in the course of the illness with astounding success.
From the day President Trump spoke about therapeutics, it seemed that the vaccine became the endgame, the ultimate remedy for a return to normalcy. It seemed as though the vaccine was the beeline toward which "everyone" was racing. And now, there are brave people out there finding that the vaccine may not be behaving as expected and, in some cases, is causing alarming vascular damage and or/death.
Please ask yourself why.
